| dc.contributor.author | Shepherd, M | |
| dc.contributor.author | Brook, AJ | |
| dc.contributor.author | Chakera, AJ | |
| dc.contributor.author | Hattersley, AT | |
| dc.date.accessioned | 2017-05-04T11:56:09Z | |
| dc.date.issued | 2017-06-13 | |
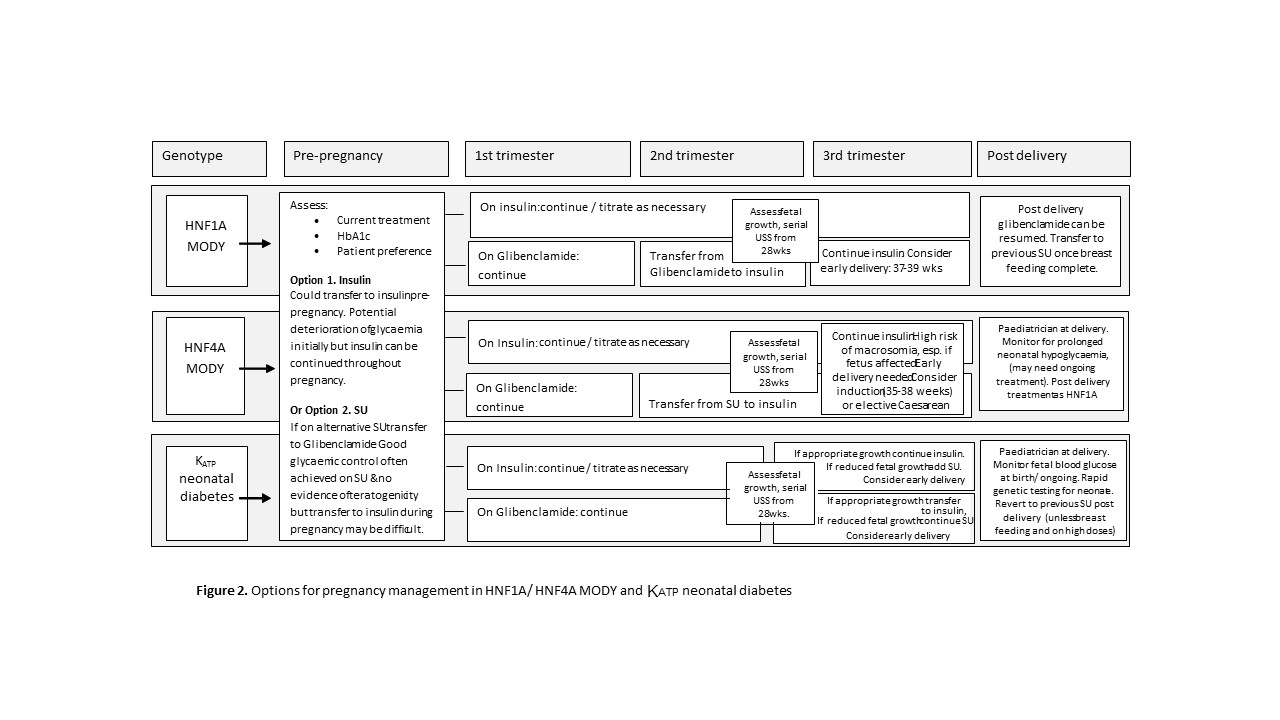
| dc.description.abstract | HNF1A/HNF4A maturity onset diabetes of the young (MODY) and KATP channel neonatal diabetes (NDM) are optimally treated with sulfonylureas outside pregnancy, but there is little evidence regarding the most appropriate treatment during pregnancy.
Glibenclamide has been widely used in the treatment of gestational diabetes, however recent data establishes that glibenclamide crosses the placenta, and increases risk of macrosomia and neonatal hypoglycaemia. This raises questions about its use in pregnancy. We review the available evidence and make recommendations for the management of monogenic diabetes in pregnancy.
Due to the risk of stimulating increased insulin secretion in utero, we recommend that in women with HNF1A/ HNF4A MODY, those with good glycaemic control on a sulfonylurea pre-conception either transfer to insulin before conception [at the risk of a short-term deterioration of glycaemic control] or continue with sulfonylurea (glibenclamide) treatment in the first trimester and transfer to insulin in the second trimester. Early delivery is needed if the fetus inherits an HNF4A mutation from either parent as increased insulin secretion results in ~800g weight gain in utero, and prolonged severe neonatal hypoglycaemia can occur post-delivery.
If the fetus inherits a KATP neonatal diabetes mutation from their mother they have greatly reduced insulin secretion in utero that reduces fetal growth by approximately 900g. Treating the mother with glibenclamide in the third trimester treats the affected fetus in utero normalising fetal growth but is not desirable, especially in the high doses used in this condition, if the fetus is unaffected.
Prospective studies of pregnancy in monogenic diabetes are needed. | en_GB |
| dc.description.sponsorship | MS is supported by the NIHR Exeter Clinical Research Facility. ATH is a Wellcome Trust Senior Investigator and NIHR Senior Investigator. This work was supported by the National Institute for Health Research (NIHR) Exeter Clinical Research Facility. The views expressed in this publication are those of the author(s). MS contributed to drafts and revised the manuscript. ATH and AJC contributed to drafts. AJB contributed to drafts and obstetric input. There are no conflicts of interest to declare. | en_GB |
| dc.identifier.citation | Vol. 34 (10), pp. 1332-1339 | |
| dc.identifier.doi | 10.1111/dme.13388 | |
| dc.identifier.uri | http://hdl.handle.net/10871/27376 | |
| dc.language.iso | en | en_GB |
| dc.publisher | Wiley for Diabetes UK | en_GB |
| dc.rights | © 2017 The Authors. Diabetic Medicine published by John Wiley & Sons Ltd on behalf of Diabetes UK. This is an open access article under the terms of the Creative Commons Attribution License, which permits use, distribution and reproduction in any medium, provided the original work is properly cited: https://creativecommons.org/licenses/by/4.0/ | |
| dc.title | Management of sulfonylurea treated monogenic diabetes in pregnancy: implications of placental Glibenclamide transfer | en_GB |
| dc.type | Article | en_GB |
| dc.identifier.issn | 0742-3071 | |
| dc.description | This is the author accepted manuscript. The final version is available from Wiley via the DOI in this record. | |
| dc.identifier.journal | Diabetic Medicine | en_GB |
{kind=link}